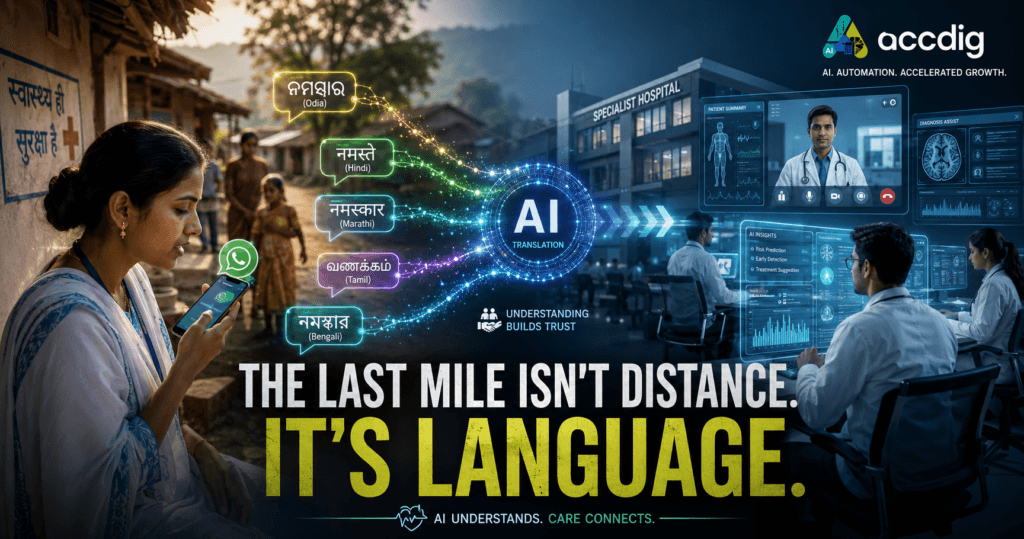
Vernacular AI in Healthcare is transforming how Bharat communicates, connects, and accesses quality medical care—turning every regional language into a bridge between patients, doctors, and better health outcomes.
Because the biggest barrier to healthcare in India isn’t always distance. Sometimes, it’s language.
The issue of the last mile in healthcare in India has been the topic of discussion for decades. It’s usually fixed in terms of distance, the distance between a village with a patient and a city with a doctor, in this case in kilometers.
In reality, the last mile that I’ve experienced is not geographic. It’s linguistic.
It is not simply a gap in information between Primary Health Centre (PHC) and the metro hospital but rather a lack of trust that arises when even a specialist during a patchy video visit, fail to understand what the patient means when he states that he has a ‘pet mein jalan’ – a burning sensation in the stomach.
This has been an enigma which tech professionals and policy makers have not been able to solve. We can build complex artificial intelligence models, but so far it doesn’t work in Bharat because it is based on English samples and urban concepts. But, that’s about to change. But there’s another type of regional-language AI in healthcare space, and one billion of infrastructure investments were not enough to demonstrate this—vernacular-first bots are doing just that.

The Great Divide: Why Vernacular AI in Healthcare Succeeds Where English-First AI Fails.
Let’s be blunt. The feeling of “feeling blue” is a very complex emotion to an AI. Now try to convey the same meaning in Marwari dialect, etc. that is between udhaas (sad) and bekaar lag raha hai (feeling useless/worn out).
The initial stages of rural health Tech revolution in India was a pastiche of the western models. It was based on the principle of being app first, English first and data intensive. It was a miss for those who needed it.
- The App Fallacy: It assumed that there will be a new app that will require a lot of space on their mobile phones, a level of digital literacy and quick internet connectivity.
- The Language Barrier: It forced users to either have to speak English or some level of stilted formal Hindi which no one actually speaks, which, in effect is like Google Translate.
- The Trust Gap: If a tool does not know you, then you do not trust it – this is the Trust Gap. In the healthcare industry, there’s nothing that can be more valuable than trust.
The times of paradigm shift are here. The new models are built around vernacular AI in healthcare, enabling more inclusive access to healthcare AI in India, and do not hard-sell the user on the technology, they hard-sell the technology on the user.
Case Study: The AI Last-Mile to Triage to Trust (Last-Mile).
This isn’t theory. This is a show that I’m seeing on a floor. The best rural health tech solution are not a futuristic robot, but the simple ones – text/voice based bots that can be found in the one app that 500 million or more Indians already use – WhatsApp.
Suppose that this AI is not a doctor, it is the most powerful medical super-translator, and the triage nurse. It is an online link between the patient and a specialist as well as an ASHA employee, demonstrating the power of robust multilingual healthcare technology.
Micro-Case 1 The Seva Bot (A Composite Model).
Let’s say that such a rural ASHA worker, Sunita exists in Odishi. She’s going to visit her family of a child who is sick. Child has acute diarrhoea.
- Old Way: Sunita goes over unta’s head. She contacts her boss who directs her to take the child to PHC 15km distant. The family loses wages, and tries to treat the family’s illness at home. The child gets so dehydrated that they are unable to survive.
- New Way: A day later, Sunita launches WhatsApp, in New Way. She leaves her message in Odia for health department’s bot.
- Bot (in Odia): Namaskar. How many years old is the child? What are the symptoms of? How many times today has the child had diarrhoea? “
- Sunita (Voice Note): “His two-year-old son has passed poop that had water in it 10-12 times since the morning. He doesn’t have milk in him any more and his eyes are sunken. “
- AI Triage: Extreme dehydration is indicated by the NLU model, which trains on the local medical vocabulary, for both “sunken eyes” and “10+ stools. It is important for multilingual healthcare technology frameworks to develop this kind of clinical understanding.
- Bot (in Odia): “Immediately please give the child ORS. I will put you in contact with a doctor at district hospital and have a free video call with him now. “
- The ‘Super-Translation’: The specialist responds very promptly with the message: “o ‘Super-Translation’: The specialist receives an instant translated and structured summary in English from the bot: Patient: 2 year old Male. Symptoms: Acute diarrhoea (10-12 stools/day). Affected Animal: One or more individual animals.Affected Animal: A single or multiple animal. Triage: URGENT.
The doctor calls the meeting with the light of knowledge. Within 2 minutes, the AI helped Sunita empower herself, screen the patient and help her to overcome the language barrier. This is a clear victory for AI in healthcare rural areas , demonstrating how multilingual healthcare technology can bridge communication gaps between patients and specialists.
Micro-Case 2: Fight against Silicosis in Rajasthan.
This is a great illustration to policy makers looking to build measurable rural health tech solutions.. Silicosis is a fatal occupational lung disease of the miners and is endemic in Rajasthan; and chest X-ray is required for diagnosis, which is not readily available in rural areas.
The economic survey (2024-25) mentioned that an innovative vernacular AI in healthcare solution based on artificial intelligence was being used by the state.
- A digital X-ray based machine learning model was trained to identify signs of silicosis.
- This AI will be used as a first step screening tool to flag the high-risk X-rays and pass them on to a human specialist.
- The Policy Masterstroke: Wizard is not in a vacuum. The portal is directly linked to Direct Benefit Transfer (DBT) portal of the state. On the confirmation of the diagnosis through the AI assistance, the patient is automatically signed up for financial assistance. Integration with state portals is crucial for scaling rural health tech solutions and strengthening vernacular AI in healthcare initiatives.
It is the best form of Health Tech Policy India: this is where AI can be used not only to diagnose, but also to cut through red tape and provide real assistance.
There is More to the Hype: The Data is Starting to Speak.
This is no fluke. Although these statistics are new, they are convincing.
- In a recent report on Healthcare Technology, artificial intelligence (AI) powered mobile technology has enabled nearly 70 percent of rural India to get access to specialist diagnostics for the first time in its history, mainly due to the developments in regional language AI in healthcare.
- Vents like Qure.ai are also performing AI reading on the chest X-rays and retina scans (when the case is DR) of remote vans and bringing in the critical cases to a point in mere minutes.
- In the insurance and administration space, one study found that the claim approval process could be 60 times quicker with the use of vernacular AI interfaces, just by reducing the level of errors in documents when claims in the rural population are involved. AI’s capabilities in healthcare don’t stop there.AI’s use in healthcare is not limited to diagnostics.
With tech leaders, the product-market fit is achieved. This secures a seemingly Return on Investment (ROI) for the policymakers when it comes to investing in Regional Language AI in rural healthcare in India.
The Checklist of the Analyst: A Guide to the deployment of Vernacular AI That Works.
There are projects that have been implemented in this space and projects that have failed in this space! The successful ones not only have a better code, but a better knowledge of the ecosystem as well.
I’m going to share my list of steps in creating any regional language AI in healthcare.
1. It is Not Translation it is Nuance.
Your model needs to be trained on the real speech on which you are working. It has to be capable of indicating vertigo, low blood pressure or even just high stress – it must be capable of telling that sir ghoom raha hai (my head is spinning). This includes building (or obtaining) hyperlocal data for your healthcare system AI for your region’s language.
2. Learn to Live with the Low-Resource Dilemma.
The Indian languages are low-resource to AI, that is, there is not enough data on which to train. There isn’t any such thing as having the best set of data. The secret of success is the use of techniques as follows:
- Transfer Learning: Fine-tuning over smaller data set (e.g., Bhojpuri or Marwari) is atypical in a strong model (e.g., Hindi) in order to be transferred to the new model under study.
- Human-in-the-Loop: It is a case in which the human experts correct the models errors as soon as the bot is deployed, and re-train the model as rapidly. The key enablers which come into the picture in this regard are the National Language Translation Mission by the government and the development of such schemes as Bharat Gen.
3. Construct in the Interface: Not Apps, WhatsApp.
Get off with attempting to make people download your app. Don’t go where your users aren’t. WhatsApp and primitive USSD based text/voice menus are that in India. The less the friction, the more the regional language AI in healthcare solutions will be adopted.
4. Human, The Anchor: Weigh in, Not Overthrow.
The most crucial mistake is to make AI an alternative to ASHA workers or local doctors. This is neither the right approach nor the right way to do it as it causes failure due to lack of trust.
The effective model is one whereby force is multiplied. The ASHA worker is an extension of formal health system, but is tech-enabled and trusted to be more powerful because of the AI. This synergy is the value added that regional language AI brings to healthcare.
The Elephant in the Room: Policy, Power and Pipe Dreams.
It is a naivety to ignore them and they are a challenge we face. As an analyst here I’d say it’s never a good idea to be optimistic without reason.
- Infrastructure: Bot won’t do anything if it has been turned off, or if the network is down. Only an approximation of 29 per cent of rural Indians can access broadband. It should be either offline or very light (text based) solutions. The most sophisticated regional language AI systems of all use require connectivity.
- Policy & Liability: In the event that the AI bot concludes the wrong diagnosis, who is responsible? The tech company? The hospital? The government? To scale on the national level, a regulatory sandbox with clarity on the standards of validation and liability of Health Tech Policy India is needed before that. The question is crucial when it comes to scaling up any regional language AI in healthcare service.
- Data Privacy: When sensitive health information is being gathered, in various languages, it’s a legal minefield and operating the DPDP Act. It is no longer up to debate that on-device processing and anonymisation should be undertaken.
- Talent: Granting the Economic Survey’s claim, the lack of talent who can understand AI and the details of public health is tremendous. A national priority has to be given to the training of regional language AI skills in healthcare.
Common Myth Busting
These are the questions that are always in my mind when I give briefing to the policy makers.
Myth: AI isn’t replacing ASHA workers or rural doctors, rather, it is complementing them.Myth: AI will replace the role of the ASHA workers or the rural doctors.
Bust: No. It will help to improve them. It does the grunt work, or the triage, documentation and translation so that the human can do what he/she does best – provide care, build trust and attend to complex cases. Changes an ASHA worker from a simple diagnostic assistant to a complex one.
Some Common FAQ’s
The answer is, NO, you don’t boil the ocean. The first step is to create models which are tuned for each of the major language families (like Hindi, Marathi, Bengali, Tamil etc.) for each region. This is where the process of co-operation with the State governments with hyper local health information can be useful. This is the way to deploy AI capabilities in regional language in the healthcare segment.
It will be more costly NOT to do it! A late diagnosis cost, overcrowding the ED or the avoidable death are a huge cost. It can be accomplished with already cloud-based AI (SaaS) models at a surprisingly low price and the benefit in a quarter (e.g., lower ER load) can pay back the system.
The Last-Mile: It is a Language, Not a Place.
Over the years, we have been trying to connect rural healthcare, physically. The evidence has been overwhelming and should be clear: digital and linguistic are the most efficient, most scalable and most cost-effective bridges!
It is not a what if scenario in the future with respect to regional language when it comes to regional language AI in healthcare. It is a current tense what works. The critical infrastructure makes the two Indias, Bharat and Urban India interconnected.
In the case of tech leaders, the difficulty lies in developing with empathy and paying attention to detail.
For the policymakers, it is all about setting the regulatory sandboxes where such tools can be safely used in a scalable way.
The code/concrete last-mile solution isn’t just a code/concrete solution. It’s about conversation. After all, long ago, our technology is now learning to converse the language, local language AI in healthcare has become a reality.
DM us on Instagram from more insights on regional language AI in healthcare.